Black Mothers, Broken System: The Maternal Mortality Gap
Structural forces like bias, unequal access to resources, and cumulative stress interact to shape pregnancy outcomes for Black women.

Read Time: 4 minutes
Published:
A heartbreaking viral video captured the experience of Karrie Jones, a Black mother who arrived at Dallas Regional Medical Center in active labor and visible distress. Filmed by her family, the footage shows Jones doubled over in a wheelchair in the waiting area while hospital staff continued asking routine intake questions rather than rushing her to labor and delivery. She waited more than 30 minutes before being admitted and gave birth just 12 minutes later. Jones and her baby were ultimately safe, but the video sparked widespread outrage and reignited concerns about delayed care and persistent racial inequities in maternal health.
The Black maternal mortality crisis is not new. For decades, Black women have been at least three times more likely to die from pregnancy-related causes than White women. In 2021, the CDC found that the maternal mortality rate for Black women reached 69.9 deaths per 100,000 live births, compared to 18.2 for White women. The disparity persists across income and education levels: Black women with college degrees remain at a higher risk than White women without a high school diploma.
Black women consistently report having their pain dismissed, their symptoms minimized, and complications such as preeclampsia or postpartum hemorrhage diagnosed too late. After giving birth by emergency C-section in 2017, Serena Williams had to repeatedly insist that doctors investigate her shortness of breath, which ultimately revealed life-threatening blood clots in her lungs.
Many Black mothers’ adverse health outcomes are linked to “weathering,” the cumulative physical toll of chronic stressors, such as discrimination, poverty, and structural racism. Over time, this stress increases Black women’s risk of pregnancy complications, including preterm birth and low birth weight. Even when financial resources are stable, Black women in the U.S. still face higher rates of pregnancy-related deaths.
Lasting change requires confronting the structural forces that endanger Black women in the first place.
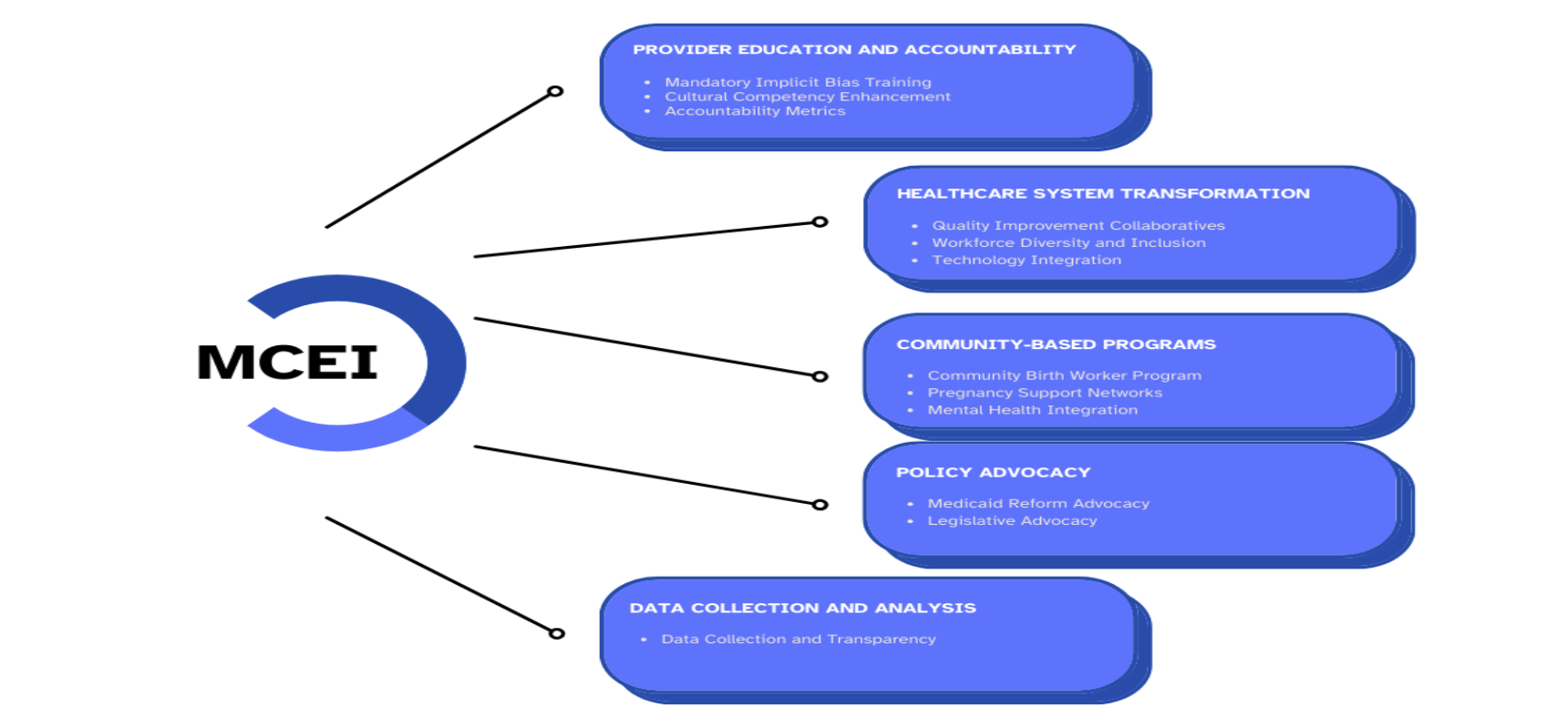
Itohan Egbedion and colleagues applied the Theory of Fundamental Causes, which frames social conditions like racism, socioeconomic status, and education as drivers of health inequalities, to explain why medical advances have failed to close the Black maternal mortality gap. Drawing on a decade of peer-reviewed studies and government data, the researchers developed the Maternal Care and Equity Intervention (MCEI) framework. The framework highlights how structural forces like institutional bias, unequal access to resources, and the cumulative stress of racism interact and continue to shape pregnancy outcomes for Black women.
Racial disparities in maternal mortality persist because structural and social conditions shape access to power, resources, and high-quality care in ways that disadvantage Black women. Reducing maternal deaths, therefore, requires addressing sociocultural, economic, and political factors that influence how care is delivered, accessed, and regulated. A key sociocultural factor is implicit bias, which can cause providers to dismiss Black women’s symptoms, leading to delayed diagnoses and inadequate treatment. Economically, maternity care deserts (or areas with few or no accessible maternal health facilities) limit access to nearby prenatal and emergency services, often forcing women to travel long distances for services. At the policy level, the absence of national standards leads to inconsistent implementation of proven strategies to reduce maternal deaths, disproportionately affecting Black women.
The MCEI framework (illustrated below) aims to address structural inequities through provider accountability, mandatory implicit-bias and cultural-humility training, standardized protocols, workforce diversification, telehealth expansion, and free doula and pregnancy support networks.
Community-based programming, such as prenatal group care, further demonstrates the power of collective support. By bringing women with similar due dates together for clinical care and peer connection, group programs have been shown to reduce preterm birth—an outcome that disproportionately affects Black women and contributes to infant mortality and long-term health strain.
National momentum is growing. In 2020, Congresswoman Lauren Underwood (D-IL) introduced the Momnibus Act, expanding funding in community-based maternal health initiatives. Yet lasting change requires confronting the structural forces that endanger Black women in the first place. Karrie Jones’s experience illustrates one of the many systemic failures that drive disproportionately high maternal mortality rates among Black women. Frameworks like MCEI highlight how comprehensive, accountable, community-centered, and respectful care can help Black mothers live longer, healthier lives.



