Making Aging Healthier
People are living longer than at any time in human history. To address the needs of our aging population, we must consider four new realities.

Read Time: 5 minutes
Published:

Making Aging Healthier
When Jeanne Calment was 90 years old she sold her apartment to a lawyer named Andre-Francois Raffray on a contingency contract. The deal was that he would pay her 2,500 francs a month (about $400) until her death, whereupon the apartment would become his. This would have been a nice arrangement for Raffray, were it not for the fact that Calment lived for another 32 years, to the age of 122—the longest human life on record.
Today, people are living longer than at any time in human history. The world population of those aged 65 and older will increase by a factor of 10 between 1950-2050, so that by the middle of the century, there will be about 2.5 times as many adults over age 65 as children under five.
To address the needs of this aging population we must consider four new realities.
First, healthy aging is the ultimate example of prevention in action. To age healthy we have to prevent disease from taking hold, suggesting a redoubled effort in preventing some of the conditions—like obesity and substance use—that result in unhealthy older life.
Second, we must create structures and communities that ensure the full participation of citizens of all ages. From advocating for more accessible built environments to pushing for more volunteer opportunities for older adults, we have a chance to redefine what aging looks like in the decades to come.
Third, we must identify and work towards mitigating health gaps that exist among aging populations. Race, for example, remains a persistent factor in determining health outcomes and life expectancy at all ages. The aging LGBTQ population also faces a distinct set of issues, while socioeconomic status remains central to the determination of health for all aging populations.
And finally, we need to intensify our efforts to tackle the health challenges that older people face. In 2006, the number of worldwide Alzheimer’s disease cases was 26.6 million; that figure is projected to quadruple by 2050, leaving one in 85 people in the world with this condition.
While worries about increasing health care costs coupled with a decline in the wage-earning population are real, we see increased longevity as the happy result of improvements in the conditions that make populations healthy. More importantly, this demographic shift presents a remarkable moment in human history we would be well-advised to recognize.
Warmly,
Michael Stein & Sandro Galea

CALORIE COUNTING
The Food and Drug Administration (FDA) requires restaurants with 20 or more locations nationwide to post calorie information as an obesity prevention policy. These researchers found that only 17% of restaurants in four large cities would therefore need to comply with the FDA’s restaurant menu-labeling law. Menu labeling is more likely to affect restaurants in higher-income neighborhoods and in non-Hispanic Black and mixed race/ethnicity areas. Since the current restaurant labeling mandate reaches so few customers, the restaurant industry would have to make additional voluntary changes to promote healthy choices in eating, such as offering smaller portions and limiting unhealthy beverages.
NEW IMAGES FOR THE VISUALLY IMPAIRED
Worldwide, hundreds of millions of people are blind or functionally blind. Traditionally, people who are blind use guide canes to detect obstacles in their path. These researchers evaluated a smartphone navigation system that continuously captures images of the environment in front of a user who is visually impaired, and performs image processing and object identification to inform the user of the image results. The system achieved a 60% recognition rate across different environments, with high recognition of buses, cars and other people, but lower rates of bicycles and potted plants. Users of the system, which is sure to improve, are able to identify objects, roughly gauge their location, and gain a more comprehensive understanding of their surroundings.

CONTRACEPTION OPTIONS LIMITED IN RURAL AND SUBURBAN AREAS
Geography can play a role in what types of contraception are available to women at their local community health centers. Women in rural and suburban areas have fewer contraception options than those in urban areas.
George Washington University and the Kaiser Family Foundation surveyed community health centers across the United States about their family planning services last year. They received responses from 546 health centers representing all 50 states and the District of Columbia.
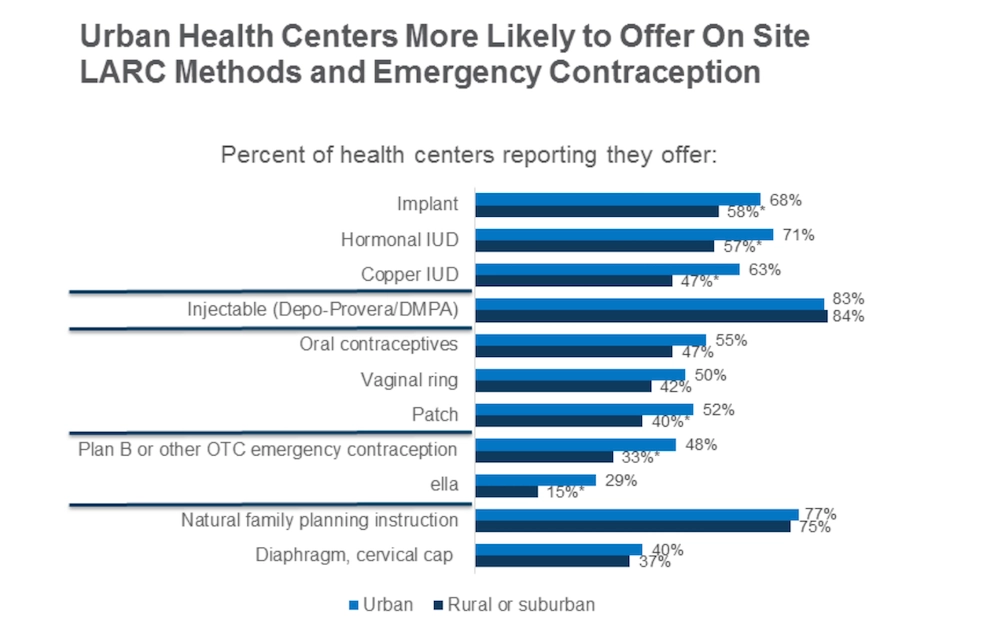
The figure shows the proportion of rural and urban health centers providing specific types of contraception. Significantly fewer rural and suburban health centers provide long-acting reversible contraception: the implant, hormonal intrauterine device, and copper IUD. This is also true for emergency contraception: over-the-counter methods such as Plan B and prescription methods such as ella.
Long-acting reversible contraception methods are highly effective forms of birth control. Once placed in the body, they can protect women for several years. Emergency contraception is a form of birth control taken after sex to prevent pregnancy. It is sometimes referred to as the “morning after pill.” Poor access to these popular and effective forms of contraception increases the risk of unintended pregnancy for women in rural and suburban areas.
Graph from Community Health Centers and Family Planning in an Era of Policy Uncertainty, Susan F. Wood, Julia Strasser, Jessica Sharac, Janelle Wylie, Thao-Chi Tran, Sara Rosenbaum, Caroline Rosenzweig,Laurie Sobel, and Alina Salganicoff, published: March 15, 2018.