Zero Tolerance for Preventable Deaths
The number of preventable causes of death is improving in the US, per Michael Stein and Sandro Galea in The Public's Health.

Read Time: 5 minutes
Published:

Zero Tolerance for Preventable Deaths
Of the approximately 150,000 daily deaths around the world, about a third, or 50,000 or so, are preventable (the rest are age-related, hence non-preventable). In the United States more than 400,000 people die annually due to smoking and more than 300,000 due to poor diet, the leading causes of preventable deaths.
The good news is that the number of preventable causes of death is improving in the US. Preventable deaths from cancer, injuries, stroke, and heart disease decreased by 25, 23, 11, and 4 percent respectively in the first five years of this decade. We also know that we can reduce the number of deaths from preventable causes further. An analysis conducted by the Centers for Disease Control and Prevention (CDC), found that if we were to reduce the number of deaths across all states to the levels found in the best three states we would save 91,891 deaths from diseases of the heart, 84,539 from cancer, 37,016 from unintentional injuries, 28,853 from chronic lower respiratory diseases, and 17,062 from stroke for a total of more than 250,000 deaths annually, or nearly 10% of annual deaths in the US.
Should it not occasion headlines that we can prevent more than a quarter million deaths a year, but choose not to? We recognize why we don’t see such headlines: it would require a tremendous effort to prevent disease, to lessen risk behaviors, and, as we have written frequently in The Public’s Health, to deal with the foundational social, economic, and environmental contexts that shape these risk factors and health. Because it will be hard, slow work, we give ourselves license to keep spending a mere 5% of our health dollars on prevention.
But let us entertain a thought exercise. There are four billion airline passengers a year worldwide. What if there were 10,000 deaths annually from air crashes? We would call these preventable—after all, most people who fly do not expect to die. And what if we knew that we could reduce these deaths if all airlines behaved like the three best. And what if we decided not to oblige the less safe airlines to make improvements, but continued to have passengers fly on them? What if we allowed the reduction of these preventable deaths to remain only an aspiration?
We would find this situation intolerable because we have zero tolerance for any deaths from flying, and find each death vexing and unacceptable. It is remarkable that we have figured out how to fly four billion people around the world annually with minimal deaths. It is equally remarkable that we are not focused on determining screening, early intervention, risk factor reduction programs and public health efforts that set the best states apart. It seems to us that we are currently conceding that we are not serious about averting preventable deaths. A zero-tolerance policy toward such deaths might spur us to action.
Warmly,
Michael Stein & Sandro Galea

SUCCESS ZONES FOR THE UNDERSERVED
The Health Enterprise Zone Initiative, a collaboration between the local health departments, hospitals, and community-based organizations in Maryland, was designed to attract primary care providers to underserved communities and provide social services to these populations. The initiative deployed community health workers and provided behavioral health care, dental services, health education, and school-based health services to address communities’ unique health needs. The authors found that the initiative reduced hospital admissions and readmissions, although it increased emergency department visits during 2013–16. The net cost savings from reduced inpatient stays far outweighed the initiative’s cost to the state, demonstrating that a coordinated approach to leveraging resources can benefit underserved communities.

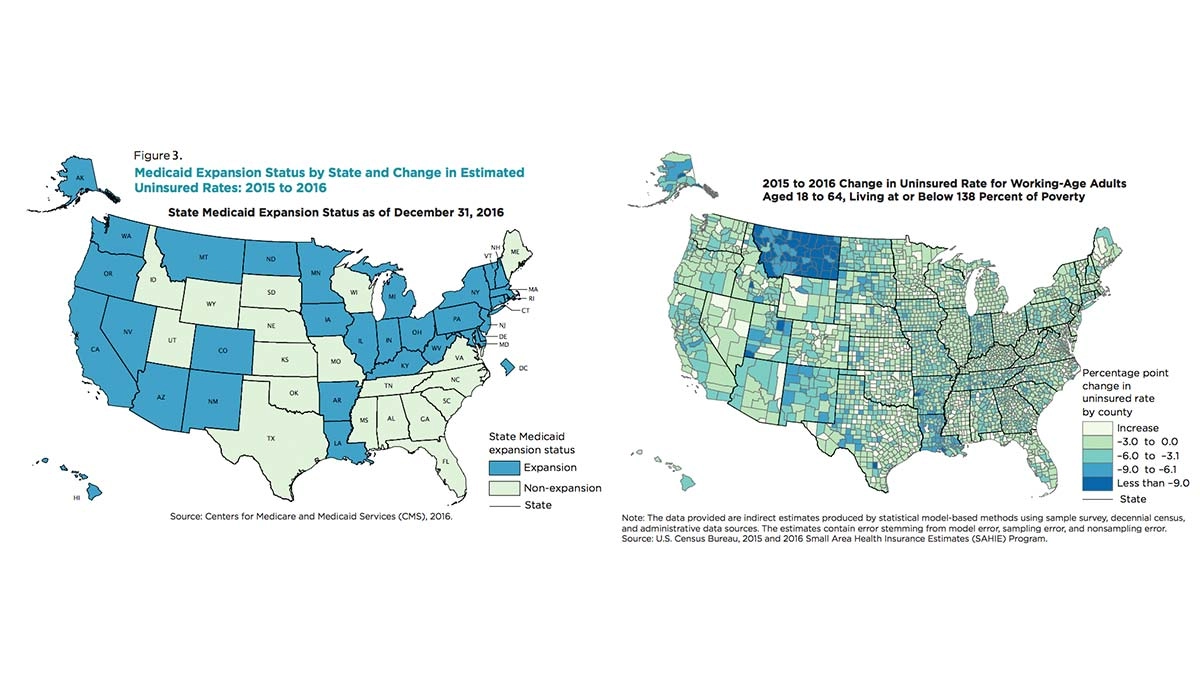
MEDICAID: 2016 UNINSURED RATES BY COUNTY
The goal of the Affordable Care Act (ACA) was to expand health care coverage, creating the closest thing to universal coverage the United States has ever seen. Many states increased coverage among previously uninsured residents by expanding Medicaid eligibility. Thirty-three states and the District of Columbia have expanded Medicaid and three more are considering expansion. The thirteen remaining states are not obligated to do so, due to a Supreme Court ruling that mandatory expansion is unconstitutionally coercive.
A report published in 2018 by Bowers, Gann, and Upton, summarizes data from the 2016 US Census Bureau’s Small Area Health Insurance Estimates program. In the map on the left, states that expanded Medicaid coverage between 2015-2016 are blue. The map on the right, shows health care coverage for low-income individuals by county. Dark blue shows that more new people were covered by health insurance out of the total potential population. In states that expanded Medicaid, 23.4% of counties saw a decrease in their estimated uninsured rates (350 counties out of 1,498). This change is substantially larger than the 5.6% decrease in states that did not expand Medicaid eligibility (92 counties out of 1,643).
Within states that expanded Medicaid, the umbrella of coverage widened through the contribution of Federal Subsidies, allowing for almost 12,000 newly-eligible Americans to gain coverage.
Maps: “Small Area Health Insurance Estimates: 2016 Small Area Estimates March 2018,” Figure 3., Lauren Bowers, Carolyn Gann, and Rachel Upton