The Public Health Spending Mismatch
We are spending more on medical, curative care, but far less than other nations on building the conditions that make people healthy.
Read Time: 2 minutes
Published:
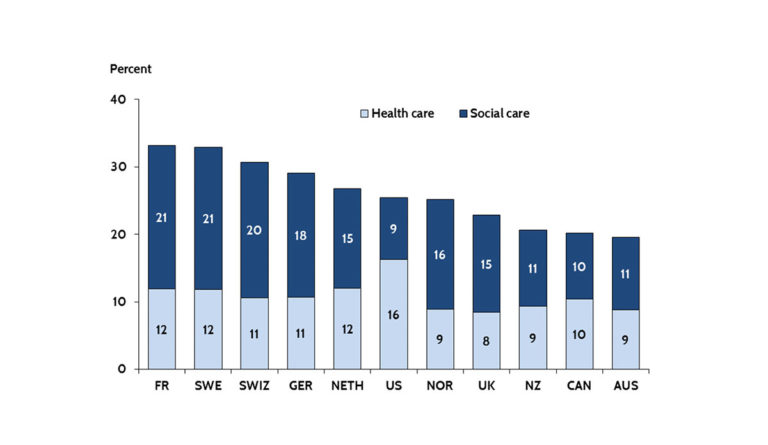
When one combines spending both on medical care (and I would argue that the light blue bar above would be better labeled “medical care” than “health care”), with a broad range of social investments in the resources that can create the health of populations (above labeled “social care”), U.S. spending is roughly in the middle of the pack compared to peer nations. We are spending more on medical, curative care, but far less than other nations on building the conditions that make people healthy.
However, if we aspire to promote the health of populations, we must therefore do so not by increasing spending, but by spending more strategically on the foundational conditions that shape the health of populations. We must focus on the social, economic, and cultural conditions that make populations healthy, moving away from the curative approach that characterizes the U.S. investment in “health” towards a greater investment in the foundational determinants of well-being.
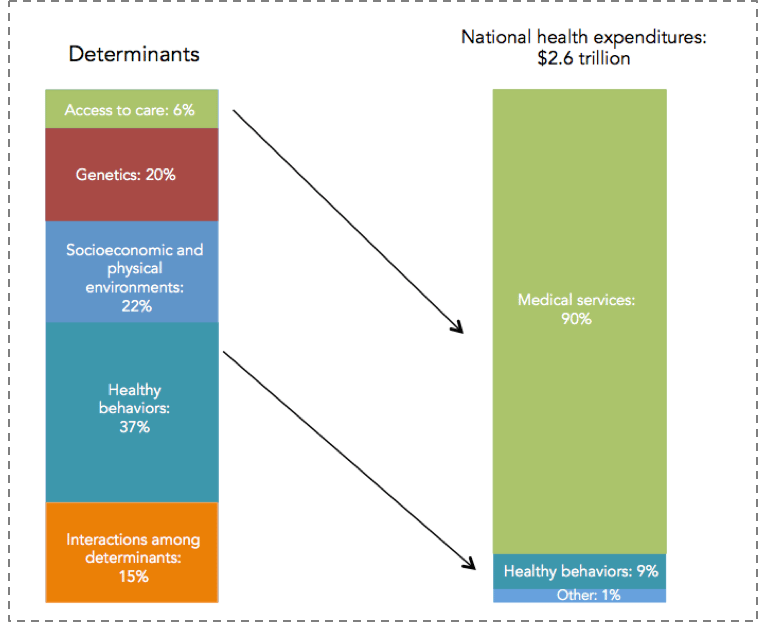
Photo via Healthy People/Healthy Economy: An Initiative to Make Massachusetts the National Leader in Health and Wellness. 2015. Data from NEHI 2013. Also featured on 18 Charts That Make the Case for Public Health, August 28, 2016.
There is no ready way of quantifying how these various levels influence health, but perhaps as good an estimate as any comes from the Network for Excellence in Health Innovation, which estimates that a large majority of health is determined by our environments and behaviors, as shown above. In this example, only about 6 percent of the production of health was attributable to medical care or access to medical care. This of course is in sharp contrast with our spending: almost 90 percent of our national health expenditure is spent on medical services.
Databyte via David Squires, US Health Care from a Global Perspective. The Commonwealth Fund.