Interpreting Medical Language Barriers
Youth who spoke languages other than English were discharged from the hospital up to 66 minutes later than English speakers, on average.

Read Time: 2 minutes
Published:
Over 68 million Americans speak a language other than English at home. In Boston alone, the top languages after English are Spanish, Haitian Creole, and Mandarin. Immigration over the last thirty years has tripled this number. Linguistic diversity enriches communities and broadens cultural understanding. But it also introduces language barriers within health care, where clear communication is critical.
Patients who face language barriers in medical exchanges experience more adverse events and require more health care services. Without adequate two-way interpretation, patients may endure increased risk of anxiety, medical errors, and worsening symptoms. For instance, non-English speakers with Type II diabetes suffer greater vision impairment than those who are fluent.
Mary Pilarz and associates conducted a retrospective analysis on how limited English proficiency affects hospital outcomes, including length of stay, discharge time, and readmissions. The study included 4,830 general medicine patients at the Children’s Hospital of Chicago from 2017-2019, categorized as English, Spanish, or other language speakers. Analyses focused on children under age 18, as they are particularly vulnerable due to limited capacity to understand care plans or self-advocate.
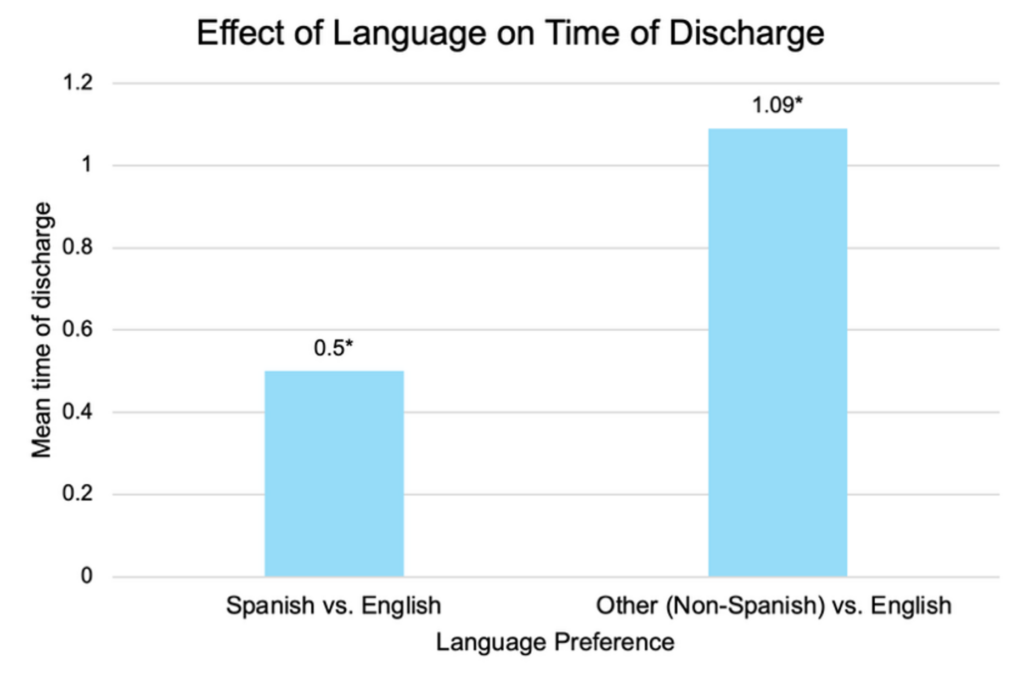
Youth who spoke Spanish or languages other than English were discharged later than English speakers. On average, Spanish speakers were discharged 30 minutes later, and other language speakers 66 minutes later. Timely discharge is essential to hospital workflow; delays can signal more complex medical needs and place additional emotional and financial stress on families. Children who spoke languages other than English or Spanish also had longer hospital stays—an average of 59 more hours (2.5 days)—and were more likely to be readmitted.
In March 2025, President Trump declared English the official national language. This executive order undermines a previous order that ensured greater access to federal services for people with limited English proficiency. In health care, the downstream effects threaten access to vital services like medical interpretation.
The study also highlights how inconsistent interpretation use may contribute to language-related disparities. Although interpretation services are available in various formats (i.e., in-person, phone, video), they remain largely underutilized in hospital settings. Time constraints and unconscious biases can deter clinicians from seeking interpretation, compromising care. A deeper commitment to culturally responsive care and meaningful investment in language access is essential to meet people where they are and bridge the communication gap across hundreds of unique languages.



