Can CEOs Save the Health of Americans?
The “right” CEO can turn around a private company’s performance profoundly. Can they do the same for health?

Read Time: 5 minutes
Published:

Can CEOs Save the Health of Americans?
We know that the health of Americans is not as good as it should be, that Americans die younger and live unhealthier lives than our high-income peers. And there are many efforts rushing in to help address this challenge, both out of a genuine interest in creating healthier populations but also perhaps out of commercial opportunity. Two of these are the moves towards health system consolidation and to the entry of large corporations like Amazon and Walmart trying to reinvent care delivery. Both of these moves depend on the private sector transforming health care, an assumption that CEOs, accountable to shareholders rather than to communities, may transform health care more quickly and thoroughly than the public sector has, or perhaps can. But is there reason to believe that CEOs, and the private sector, can create healthier populations?
Over the past 50 years, the cultural reputation of the corporate CEO has soared; the “right” CEO can turn around a private company’s performance profoundly, many believe. More recently we’ve extrapolated this belief to examples in the public sector—a principal can transform a school, a top manager can take an NGO to a new level. But the evidence that the CEO and the private sector can actually be a force for good health is far more dubious.
In the 1980s the British government decentralized its health care management model and CEOs were given full responsibility for the administration and performance of individual public hospitals and individual hospital boards could now select and reward individual CEOs. Frequent movements of CEOs seeking salary increases across British hospitals followed, providing an ideal setting to study whether individual CEOs improved hospital performance.
A recent study found that while a CEO could affect certain aspects of his or her environment—growth in number of beds, job satisfaction of staff—the person at the top did not affect health outcomes.
In some ways this shouldn’t have come as a surprise. Hospitals are wildly complex. They have thousands of diagnoses to contend with, thousands of procedures or “products.” A CEO, even if she is a physician, cannot keep up with all her products, and so in a sense she is flying blind. Here in the United States—where the success of “star” health system CEOs has never been proven—there is the added difficulty that payment for service is dependent on external forces, in particular contracts with insurers.
This points to the real problem with a CEO takeover of health care as a way of improving health. In health the outcome of interest is, well, health, and that outcome depends on much more than the forces that drive the fiscal wellbeing of the organization, i.e, the measure over which the CEO has control. Improvement in the health of a population takes time and therefore the rules of the private sector, where CEOs are rewarded for short-term performance as our stock market dictates, should be refused.
Warmly,
Michael Stein & Sandro Galea

THE HELP AND HARM OF BENZOS
Benzodiazepines, effective when used as prescribed for treating anxiety and insomnia, are often taken in conjunction with opioids and contribute to the addiction epidemic that has increased overdoses in the US. These medications are commonly misused and can present their own risks, including traffic accidents, memory problems, and depression. These authors report that benzodiazepine use and misuse is seen more often among Whites than in racial minorities. Benzodiazepines are the latest prescription medications that probably both help (reduce anxiety) and hurt (contribute to overdose) the White American population disproportionately.

CLARIFYING MEDICAL BANKRUPTCY
Medical bankruptcy is a much-debated topic, with most questions focused on exactly how many people file for it and how often it occurs. In 2005, Elizabeth Warren and her colleagues found medical costs led to over 40% of bankruptcies in the United States. This was followed by an update in 2009, pushing the proportion of bankruptcies due to medical expenses to 62%.
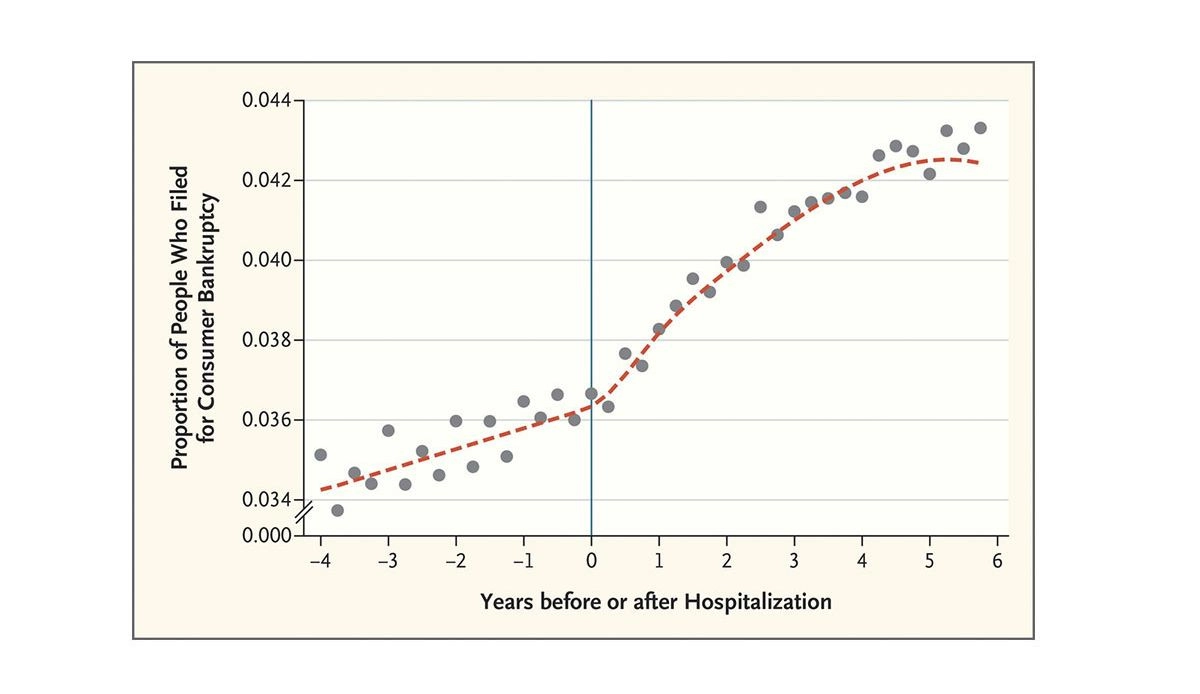
The Consumer Financial Protection Bureau’s 2014 report conflicts with this, citing that less than 1% of US adults file for bankruptcy even though 20% of the population has great medical debt. A group of economists recently reexamined this issue, concerned that the discrepancies in statistics were causing a misunderstanding of the problem. They studied a group of patients at a California hospital and looked at how hospital visits related to bankruptcy timing.
The image above shows an increase in people filing for bankruptcy after hospitalization, particularly between one and four years after admission. The researchers suggest that paying for medical bills out of pocket, and losing income because of missed work are key reasons people file for personal bankruptcy. The graph also shows, however, that only 4% of the bankruptcies were related to hospitalization, an association of much smaller magnitude than previously understood.
Warren and colleagues critiqued the economists’ research, stating that focusing only on hospitalization does not account for other medical experiences and expenses like spending time and money in emergency departments, and paying for chronic illness treatments. The economists’ subsequent response argued that estimating a causal relationship requires focusing on an isolated factor, like hospitalization. —Sampada Nandyala, PHP Fellow
Graph from New England Journal of Medicine, “Myth and Measurement — The Case of Medical Bankruptcies” by Carlos Dobkin, Amy Finkelstein, Raymond Kluender, and Matthew J. Notowidigdo, March 22, 2018.